
The Mallampati Classification and Digital Medical History: Why Airway Assessment Remains the Domain of the Clinic
The Mallampati classification is a visual examination of the oral cavity performed by a trained professional directly on a seated patient—it cannot be assessed using a digital questionnaire. medudoc therefore supports airway assessment in the areas where intelligent digital medical history-taking excels: in the structured collection of medical history and in providing early, personalized information about anesthesia procedures and alternatives. The physical airway examination itself—including the Mallampati classification—continues to be performed in person by the physician during admission.
What is the Mallampati classification, and what is it used for?
The Mallampati classification (in the form commonly used today, as modified by Samsoon and Young) assesses, based on the visibility of the soft palate, the uvula, and the palatal arches when the mouth is open to assess how well the larynx is likely to be accessible during a subsequent laryngoscopy. It is one of several predictors of difficult mask ventilation or intubation and is used during daily premedication rounds.
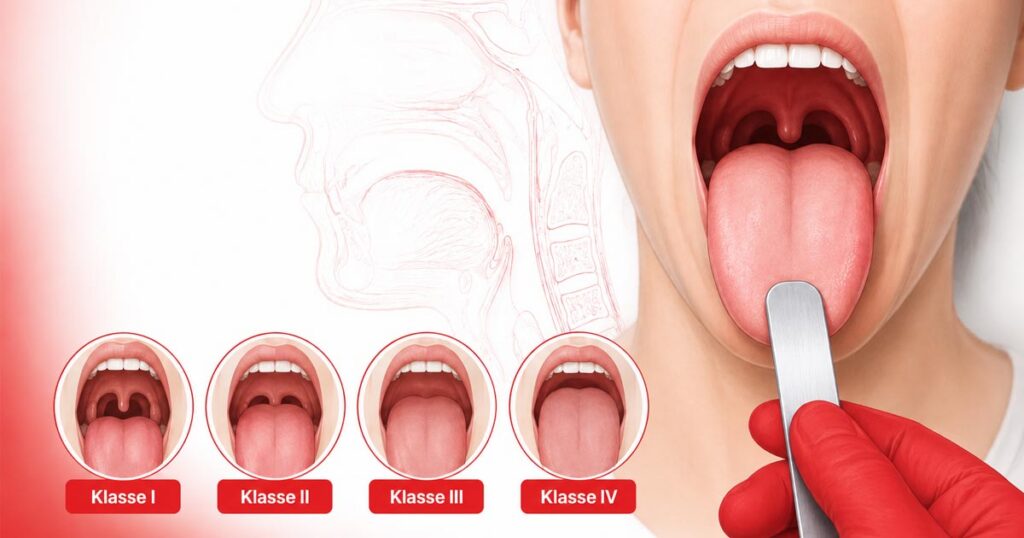
The four degrees are distinguished as follows:
- Grade I — the soft palate, uvula, and both lateral palatal arches are fully visible.
- Class II — the lateral palatal arches and the tip of the uvula are no longer visible.
- Grade III — only the soft and hard palates are visible.
- Grade IV — only the hard palate is visible.
The S1 guideline “Airway Management” from the German Society of Anesthesiology and Intensive Care Medicine (DGAI) points out that the Mallampati classification alone has limited predictive value and becomes more reliable when combined with the Patil thyromental distance (reference value below 6–7 cm). The guideline also identifies known weaknesses in its practical application—even by experienced anesthesiology staff.
Why can’t the Mallampati classification be determined through a digital medical history?
The Mallampati classification requires a direct visual examination by a trained individual—head position, mouth opening, tongue protrusion, and lighting all influence the result, and even among experienced examiners, the classification varies. A self-photo or a description provided by patients cannot replicate these examination conditions.
The DGAI guideline also explicitly places the assessment of anatomical and physiological indicators of difficult mask ventilation or intubation within the context of the pre-anesthesia evaluation—that is, the clinical examination performed by the physician, not the patient’s medical history. In addition to the Mallampati classification, these include, among other things, mouth opening, dental status, mandibular protrusion, and cervical spine mobility.
Specifically, this means that medudoc digitizes the medical history—that is, the information patients can provide themselves (previous anesthesia-related issues, anesthesia record, known intubation difficulties, sleep apnea diagnosis). The physical examination of the respiratory tract remains a medical procedure that can only take place during an in-person visit.
What does the specific process at medudoc look like—from taking a medical history at home to a respiratory examination at the clinic?
The digital preoperative workflow makes a structured distinction between information that can be collected from the patient and examination findings that must be recorded by the physician, both of which are consolidated into the same structured medical record.
- At home, by patients: The adaptive digital medical history form collects information on pre-existing conditions, previous anesthesia experiences, known respiratory issues, signs of sleep apnea, and medications. Follow-up questions dynamically adapt to the answers provided.
- First, via video: Patients watch the personalized informational video about the planned anesthesia procedure—at their own pace and with the option to rewatch sections on alternative procedures.
- In the HCP Dashboard, by medical staff: The structured medical history data is prepared and available before the appointment, including a completeness status and configurable alerts.
- During the initial assessment by the healthcare professional: In the “Airway & Anatomy” module, examination findings are documented in a structured manner—including the Mallampati classification, mouth opening, thyromental distance, cervical spine mobility, and dental status. This is an existing feature of the medudoc platform (as of May 2026).
- For the physician performing the intubation: Immediately before induction of anesthesia—in accordance with guidelines and regardless of any previous steps—the physician must perform their own assessment of the airway.
| Before the recording (digital, by patients) | Upon admission (at the hospital, by a member of the medical staff) |
|---|---|
| Medical history regarding previous anesthesias and respiratory problems | Mallampati Classification (Grades I–IV) |
| Signs of sleep apnea, dental prostheses, previous surgeries in the head and neck region | Mouth opening (interincisal), thyromental distance |
| Information on Anesthesia Procedures and Alternatives via Video-Assisted Patient Education | Mobility of the cervical spine (reclination/inclination) |
| Structured Transfer of Data to the HCP Dashboard | Dental status, risk factors for difficult mask ventilation |
| — | Repeat airway assessment immediately before induction of anesthesia (mandatory, in accordance with guidelines) |
What are the legal frameworks governing medical history, airway assessment, and patient education in Germany and Austria?
In Germany, taking a medical history is part of the obligations under the treatment contract, while the duty to provide information is codified in the Patient Rights Act. In Austria, there is no nationwide codification of a Patient Rights Act; the relevant laws are the Medical Practitioners Act, general tort law, and specialist medical guidelines that are recognized as federal quality guidelines.
Germany
- Section 630a of the German Civil Code (BGB) governs the treatment contract and, thereby, the obligation to conduct a thorough medical history as the basis for any treatment.
- Section 630e of the German Civil Code (BGB) governs the duty to provide information: It must be provided in a comprehensible manner, in a timely fashion, and tailored to the individual. Paragraph 2, No. 1 expressly requires a face-to-face conversation between a healthcare professional and the patient—digital tools can help prepare for this conversation, but cannot replace it.
- The DGAI’s S1 guideline on “Respiratory Tract Management” is not a law, but rather a consensus among medical specialists (AWMF classification S1). It describes the recognized state of medical science and is therefore relevant to the question of what standard of care is applied in liability matters.
Austria
- Section 51 of the 1998 Medical Practitioners Act governs the documentation requirements and includes the medical history as well as the content of the informed consent discussion; standardized informed consent forms are permitted, but must be tailored to the individual patient.
- The preoperative evaluation follows the ÖGARI source guideline “Preoperative Patient Evaluation, ” which is recognized by the Federal Health Commission as a Federal Quality Guideline (BQLL).
- The ÖGARI information sheet “The Difficult Airway” is available specifically for cases involving a difficult airway.
Both German and Austrian law agree on one key point: Standardized or digital informed consent materials are permitted and even expressly provided for—but they must be individually tailored to each patient, and a face-to-face conversation remains a mandatory part of the process. You can also find country-specific guidance for Austrian hospitals in our article on informed consent in Austria, and further background information on the German market in the legal framework for Patient Education.
How can sex education remain personalized when a sex education video is used?
The personalization of patient education does not depend on whether a video or a conversation is used, but rather on whether the content is tailored to the specific patient and whether a personal conversation takes place. At medudoc, educational videos and IC Sheets are generated individually for each patient based on their medical history, type of procedure, and risk profile—generic content is the exception, not the standard.
This creates opportunities for added value, particularly when it comes to airway issues: If the medical history suggests a potentially difficult airway (e.g., previous intubation problems or sleep apnea), the video sent in advance can inform the patient at home—without time pressure—about anesthesia procedures and possible alternatives, such as regional anesthesia. This is in line with the ÖGARI’s professional recommendation to actively educate patients about the benefits of regional anesthesia when a difficult airway is suspected. The video does not replace the mandatory in-person consultation—it allows the consultation to be more focused, as the basics are already known, leaving more time for individual questions.
Where does the physician’s responsibility lie in this workflow?
The final medical decision—including the assessment of the airway and the choice of anesthetic technique—remains entirely with the physician. medudoc organizes medical history data for the physician’s assessment and is not a medical device as defined by the MDR.
This applies regardless of the level of digitization: Even without a digital medical history, airway assessment on the day of the premedication visit is not a one-time step. The DGAI guideline stipulates that airway security must be reassessed by the intubator immediately before induction of anesthesia—regardless of what was previously documented in the outpatient clinic or during the admission interview. A structured digital medical history does not alter this ultimate medical responsibility; it ensures that the treating physician enters this assessment with better-prepared preliminary information.
Frequently Asked Questions About the Mallampati Classification in Digital Medical History Taking
Sources: DGAI/AWMF S1 Guideline “Airway Management” (Registration No. 001-028, as of August 21, 2023) · ÖGARI Source Guideline “Preoperative Patient Evaluation” (BQLL) · ÖGARI Information Compact “The Difficult Airway” (2020) · Sections 630a, 630e of the German Civil Code (BGB) · Section 51 of the Medical Practitioners Act of 1998 (Austria)





